Introduction
Changing behavior is a complex process that many individuals struggle with, whether it’s quitting smoking, adopting a healthier lifestyle, or breaking any other unwanted habit. The Transtheoretical Model (TTM), also known as the Stages of Change Model, offers a framework for understanding and facilitating behavior change. Developed by James O. Prochaska and Carlo Di Clemente in the late 1970s, this model has become a cornerstone in health psychology and behavior change interventions.
In this comprehensive guide, we’ll explore the Transtheoretical Model in depth, discussing its stages, processes, and applications. Whether you’re a healthcare professional, a therapist, or someone looking to make personal changes, understanding the TTM can provide valuable insights into the process of behavior change.
What is the Transtheoretical Model?
The Transtheoretical Model posits that behavior change is not a single event but a process that unfolds over time through a series of stages. It integrates key constructs from other theories to create a comprehensive model of change that can be applied to a variety of behaviors, populations, and settings.
The model is “transtheoretical” because it incorporates processes and principles from different theories of intervention, making it a more holistic approach to behavior change.
Learn more about the origins of the Transtheoretical Model
The Six Stages of Change
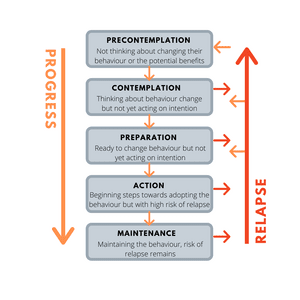
The TTM identifies six stages of change that individuals typically progress through when modifying behavior:
- Precontemplation
- Contemplation
- Preparation
- Action
- Maintenance
- Termination
Let’s examine each stage in detail:
1. Precontemplation
In this stage, individuals are not intending to take action in the foreseeable future, typically measured as the next six months. They may be unaware that their behavior is problematic or have little to no desire to change.
Characteristics:
- Lack of awareness about the need for change
- Resistance to suggestions about changing behavior
- Focus on the cons of changing behavior
Intervention strategies:
- Raise awareness about the behavior and its consequences
- Provide information without pushing for immediate change
- Encourage self-exploration and risk assessment
2. Contemplation
Individuals in the contemplation stage are intending to change in the next six months. They recognize that their behavior is problematic and are seriously thinking about changing but haven’t yet made a commitment to take action.
Characteristics:
- Ambivalence about change
- Weighing the pros and cons of changing
- Gathering information about potential change strategies
Intervention strategies:
- Help weigh the pros and cons of current behavior and change
- Boost confidence in the ability to change
- Identify barriers to change and strategies to overcome them
3. Preparation
In the preparation stage, individuals are ready to take action within the next 30 days and have typically taken some significant action in the past year. They have a plan of action, such as joining a health education class, consulting a counselor, or buying a self-help book.
Characteristics:
- Commitment to change
- Small behavioral steps towards change
- Developing a specific plan for change
Intervention strategies:
- Help develop a concrete action plan
- Set gradual goals
- Provide social support for the change
4. Action
The action stage is where individuals have made specific overt modifications in their lifestyles within the past six months. Because action is observable, behavior change often has been equated with action in the past.
Characteristics:
- Active modification of behavior
- Acquisition of new healthy behaviors
- Significant commitment of time and energy
Intervention strategies:
- Provide strategies for coping with triggers and stress
- Offer continuous support and positive reinforcement
- Help restructure the environment to support new behaviors
5. Maintenance
Maintenance is the stage in which people work to prevent relapse and consolidate the gains attained during the action stage. This stage extends from six months to an indeterminate period past the initial action.
Characteristics:
- Sustained change over time
- Integration of new behavior into lifestyle
- Ongoing vigilance against relapse
Intervention strategies:
- Develop coping strategies for high-risk situations
- Reinforce internal rewards for maintaining change
- Provide strategies for avoiding slips or relapses
6. Termination
In this stage, individuals have zero temptation and 100% self-efficacy. They are sure they will not return to their old unhealthy habit as a way of coping.
Characteristics:
- No temptation to relapse
- Complete confidence in ability to maintain change
- New behavior is fully integrated into lifestyle
Intervention strategies:
- Celebrate success
- Reinforce new self-image
- Encourage individuals to become advocates or mentors for others
Explore more about the stages of change
Processes of Change
The TTM also describes ten processes of change, which are covert and overt activities that people use to progress through the stages. These processes provide important guides for intervention programs, as they help people make and maintain change.
- Consciousness Raising: Increasing awareness about the causes, consequences, and cures for a particular problem behavior.
- Dramatic Relief: Experiencing and expressing feelings about one’s problems and solutions.
- Self-Reevaluation: Assessing how one feels and thinks about oneself with respect to a problem.
- Environmental Reevaluation: Assessing how one’s problem affects the physical and social environments.
- Self-Liberation: Making a firm commitment to change.
- Social Liberation: Increasing social opportunities or alternatives, especially for people who are relatively deprived or oppressed.
- Counterconditioning: Substituting healthier alternative behaviors and cognitions for the problem behavior.
- Stimulus Control: Removing cues for unhealthy habits and adding prompts for healthier alternatives.
- Contingency Management: Increasing the rewards for the positive behavior change and decreasing the rewards of the unhealthy behavior.
- Helping Relationships: Seeking and using social support for the healthy behavior change.
Read more about the processes of change
Key Concepts in the Transtheoretical Model
Decisional Balance
Decisional balance reflects the individual’s relative weighing of the pros and cons of changing. It involves:
- Pros: The advantages of changing the behavior
- Cons: The disadvantages of changing the behavior
As individuals progress through the stages of change, the balance typically shifts in favor of the pros.
Self-Efficacy
Self-efficacy is the situation-specific confidence that people have that they can cope with high-risk situations without relapsing to their unhealthy or high-risk behavior. This concept is based on Bandura’s self-efficacy theory and is incorporated into the TTM to help understand how people progress through the stages of change.
Temptation
Temptation reflects the intensity of urges to engage in a specific behavior when in difficult situations. It’s the flip side of self-efficacy and can be thought of as the strength of tendencies to engage in the problem behavior.
Learn more about self-efficacy and its role in behavior change
Applications of the Transtheoretical Model
The TTM has been applied to a wide range of health and mental health behaviors, including:
- Smoking Cessation: One of the original applications of the model, with numerous studies demonstrating its effectiveness.
- Weight Control and Obesity: The TTM has been used to design interventions for promoting healthy eating and physical activity.
- Substance Abuse: The model has been applied to various forms of substance abuse, including alcohol and drug addiction.
- Stress Management: TTM-based interventions have been developed to help individuals better manage stress.
- HIV Prevention: The model has been used in HIV prevention programs to promote safer sex practices.
- Medication Adherence: TTM principles have been applied to improve adherence to medication regimens.
- Domestic Violence Prevention: The model has been adapted for interventions aimed at reducing domestic violence.
Explore more applications of the Transtheoretical Model
Strengths and Limitations of the TTM
Strengths
- Comprehensive Framework: The TTM provides a comprehensive view of behavior change that integrates various theoretical perspectives.
- Flexibility: It can be applied to a wide range of behaviors and populations.
- Stage-Matched Interventions: The model allows for tailored interventions based on an individual’s readiness to change.
- Recognition of Relapse: The model acknowledges that relapse is a normal part of the change process, reducing stigma and encouraging continued efforts.
Limitations
- Discrete Stages: Some critics argue that the stages may not be as discrete as the model suggests, with individuals potentially being in multiple stages simultaneously.
- Time Frames: The specific time frames associated with each stage (e.g., six months for contemplation) may not apply universally.
- Cultural Considerations: The model may not fully account for cultural differences in the change process.
- Complexity: The model’s comprehensiveness can make it challenging to implement in some settings.
Implementing the Transtheoretical Model
To effectively use the TTM in behavior change interventions, consider the following steps:
- Assessment: Determine the individual’s current stage of change using validated assessment tools.
- Stage-Matched Interventions: Design interventions that match the individual’s current stage of change.
- Process Utilization: Incorporate appropriate processes of change based on the individual’s stage.
- Continual Reassessment: Regularly reassess the individual’s stage and adjust interventions accordingly.
- Address Multiple Behaviors: When appropriate, consider addressing multiple related behaviors simultaneously.
- Promote Self-Efficacy: Incorporate strategies to enhance self-efficacy throughout the change process.
- Prepare for Relapse: Include relapse prevention strategies, especially in the action and maintenance stages.
Find resources for implementing the TTM
Conclusion
The Transtheoretical Model offers a comprehensive framework for understanding and facilitating behavior change. By recognizing that change occurs in stages and integrating various psychological processes, the TTM provides a flexible and practical approach to behavior modification.
Whether you’re a healthcare provider designing interventions, a therapist working with clients, or an individual seeking personal change, the insights provided by the TTM can guide you through the complex process of behavior change. Remember that change is rarely linear, and progress may involve moving back and forth between stages. The key is to use the appropriate strategies for each stage and to maintain a long-term perspective on the change process.
As research continues to refine and expand the model, the TTM remains a valuable tool in the field of behavior change, offering hope and guidance to those seeking to improve their health and well-being.